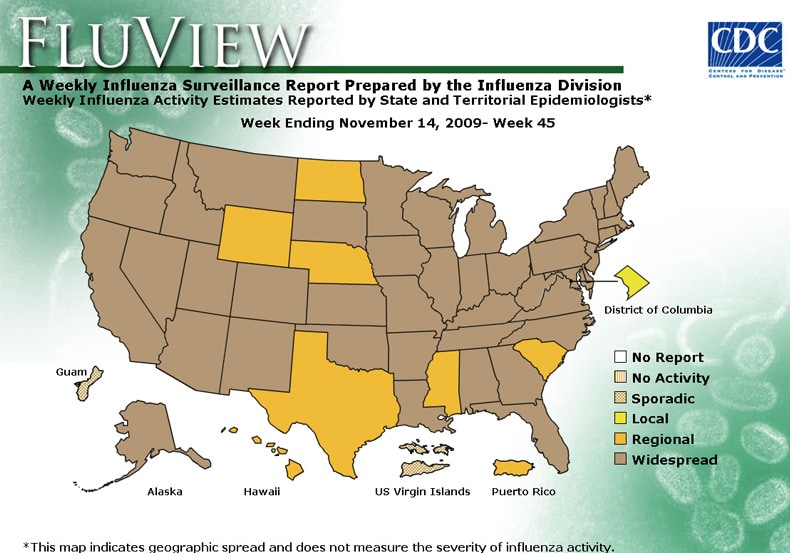
Forty-one states are reporting widespread influenza activity at this time according to the CDC. They are: Alabama, Alaska, Arizona, Arkansas, California, Colorado, Delaware, Florida, Georgia, Idaho, Illinois, Indiana, Iowa, Kansas, Kentucky, Louisiana, Maryland, Minnesota, Mississippi, Missouri, Montana, Nebraska, Nevada, New Hampshire, New Mexico, New York, North Carolina, North Dakota, Ohio, Oklahoma, Oregon, Pennsylvania, South Dakota, Texas, Tennessee, Utah, Virginia, Washington, West Virginia, Wisconsin, and Wyoming.
Last month the CDC released a guide to business to prepare for the threat of the Flu. Despite the fact that the CDC has directed ill healthcare workers to stay home, workers’ compensation commentators continue to infer that Flu claims should be absolutely defended, and in fact, ill healthcare workers and sick employees should be held to a higher standard of proof to obtain benefits.
As challenges to mandatory vaccination programs meander thorough the courts, and voluntary/mandatory absenteeism programs are implemented, the ability of the system to quickly reimburse wages for lost time from work and provide medical benefits for treatment of the contagious disease, remains questionable. Should claims be filed by even a percentage of those workers who become ill, the system, which itself is anticipated to be overtaxed, may not be able the handle the volume on an emergent basis.
So far there has been silence about workers’ compensation flu pandemic planning. While the Federal and State governments have rules and regulations in their arsenal to meet the challenge, this is an issue where workers’ compensation should be first in line to deliver benefits to sick workers.